THYROID NODULES
Thyroid nodules are among the most common thyroid disorders and are particularly common in women. Above a certain size, they can cause discomfort. Often, surgery is recommended, in which large parts of the organ or even the entire thyroid gland is removed. This may not always be necessary for benign nodules.
HOW DO THYROID NODULES DEVELOP?
The most common cause of thyroid nodules is iodine deficiency. The thyroid gland needs iodine for the production of thyroid hormones. This micronutrient is normally ingested with food and, in addition to iodized table salt, is found in fish, seafood, algae and dairy products. In Switzerland, the frequency of iodine deficiency struma has decreased significantly, as table salt has been enriched with iodine since 1922. Older people are therefore more often affected by thyroid nodules because iodine supply used to be worse in the past. If the iodine intake through food is not sufficient, the thyroid gland tries to compensate for the iodine deficiency by growing. Often, only individual areas in the thyroid gland grow - thyroid gland nodules, which are referred to as "nodular goiter", develop. More rarely, however, this can also lead to a pronounced, diffuse enlargement of the entire thyroid gland. Then it is referred to as a goiter.
HOW OFTEN ARE THYROID NODULES MALIGNANT?
In over 95% of cases, thyroid nodules are benign. Clinically relevant thyroid carcinoma is rare and its mortality low. The world's largest cancer register study (SEER program, National Cancer Institute's Surveillance, Epidemiology and End Results) found an increase in the incidence of thyroid cancer from 2.7/100,000 to 7.7/100,000 over a period of 30 years. Almost half of these carcinomas were less than 1 cm and therefore not clinically relevant. During this period, the mortality rate of thyroid carcinoma remained equally low at approximately 0.5 deaths/100,000. The study very well reflects the problem of thyroid sonography, which is available everywhere nowadays, whereby many clinically irrelevant thyroid nodules are discovered, which can often represent a diagnostic, therapeutic and emotional challenge for the physician and especially the patient.
WHAT COMPLAINTS INDICATE THYROID NODULES?

Small thyroid nodules are usually asymptomatic and often result from incidental findings during an ultrasound examination. However, larger nodules can also cause discomfort in addition to the obvious cosmetic problem. These are very variable and range from localized pain, globus pharyngis (lump in the throat sensation), voice changes, hoarseness, increased clearing of the throat to difficulties breathing and swallowing. Pressing directly on it can also cause pain. If the nodule produces hormones uncontrollably, this can lead to hyperthyroidism. The following complaints may occur: Weight loss despite good appetite, restlessness, fast pulse, tremors, diarrhea, and excessive
Indications of thyroid enlargement:
• Pressure or lump sensation in the throat
• Voice changes, hoarseness
• Difficulty breathing and swallowing
WHEN SHOULD THYROID NODULES BE EXAMINED?
Even if most of the nodules are benign, newly discovered thyroid nodules should still be carefully examined. The aim here is to rule out a rare malignant thyroid gland nodule as well as a hyperfunction. However, most thyroid nodules exhibit a normal (euthyroid) metabolism. In addition, it should be assessed whether a benign nodule is medically significant, as it is responsible for local complaints that may not have been associated until then. Often, benign thyroid nodules also exhibit relevant growth behavior, which may necessitate treatment at a later stage.

HOW IS THE EXAMINATION OF THYROID NODULES CARRIED OUT?
With a detailed anamnesis, the questioning of the patient about his medical history, as well as a reasonable pre-diagnosis, the malignancy of a thyroid nodule can be excluded in many cases. The following examinations are part of thyroid diagnostics:
Blood Test:
With a detailed anamnesis, the questioning of the patient about his medical history, as well as a reasonable pre-diagnosis, the malignancy of a thyroid nodule can be excluded in many cases. The following examinations are part of thyroid diagnostics:
Ultrasound examination (sonography):
Is regarded as a standard imaging examination in which a whole range of morphological criteria such as size, limitation, tissue structure, presence of calcifications as well as degree of blood circulation can be assessed. A very experienced physician can differentiate between benign and malignant thyroid nodules quite well on the basis of sonography.

Assessment of the blood flow of a solid thyroid nodule by duplex sonography.
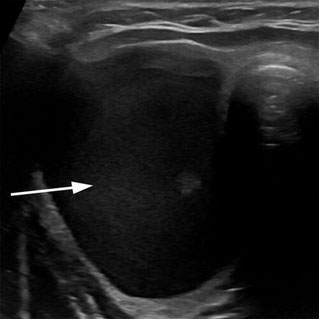
Sonographic imaging of a thyroid nodule with predominantly liquid (cystic) parts (arrow). This type of thyroid nodule is particularly suitable for minimally invasive treatment with thermal ablation.
Scintigraphy:
Is a nuclear medical examination method in which a weakly radioactively labelled iodine variant is injected into the bloodstream, which is subsequently absorbed by the thyroid tissue and can be visualized. Areas in which iodine accumulates more frequently appear yellow and red in the imaging, i.e. in warm colours. Those where there is only little marked iodine are blue-violet and therefore look rather "cold". The distinction between thyroid nodes in "hot" and "cold" therefore has nothing to do with temperature. Rather, the focus is on the activity of the nodes, i.e. whether they produce hormones or not.

Proof of unifocal operational autonomy (lower thyroid pole left in image) by 99mTc scintigraphy. Such "hot" nodules are always benign and can be treated with radioiodine therapy or thermal ablation as an alternative to surgery.
Fine needle puncture:
This is a small intervention comparable to a syringe puncture. A very thin needle is used to extract cells from the thyroid gland node, which are then examined under the microscope for potential abnormalities. The negative predictive value is 98-99%, i.e. the malignancy risk for a negative FNP finding is practically non-existent. After ruling out a dysfunction of the thyroid gland using TSH and ultrasound imaging, fine needle puncture (FNP) is the most important diagnostic procedure and should be performed additionally for cold nodes from a node size of 1.5 cm. The result obtained by FNP is an important criterion in deciding whether a thyroid gland node needs to be surgically removed or whether thermal ablation is a minimally invasive treatment alternative.